A massive U.S. study rooted in the 1960s found a classic autism rate of about .066%. Today, rates for severe autism are about 10-fold higher, and 28-fold higher for all ASD. Revisiting the study’s original data would reveal the truth about autism’s increasing prevalence.

Was autism just as prevalent in the 1960s as today? The author explains that there’s an easy way to find out. (Stock photo)
By Jill Escher
Debates over autism prevalence continue to rage. Has the rate of objectively measurable neurodevelopmental disability been increasing, or has the autism explosion been entirely subjective, as a mere matter of perception or artifact of shifting diagnostics and awareness? In other words, have 1 in 54 U.S. children always suffered the impairments of autism spectrum disorder as defined today, or were earlier generations in fact neurodevelopmentally healthier?
Believe it or not, there’s an easy way to settle this dispute. The method lies in a trove of data, mostly from the 1960s, collected by a massive U.S. government funded research project called The Collaborative Perinatal Project, or CPP.
As the nation mourned JFK and the Beatles played Shea Stadium, CPP researchers were busy gathering data for one of the largest and broadest epidemiological studies in American history. It was conceived in the 1950s as a way to better understand the causes of cerebral palsy and intellectual disability, though it also examined anatomical birth defects and other endpoints.
The CPP enrolled 55,000 pregnant mothers at 12 university-affiliated hospitals across the U.S. from 1959 to 1965. It compiled exhaustive amounts of data about the mothers and their pregnancies, and also, for 30,000 of the offspring, the health and developmental outcomes — with particular attention to thorough psychological and neurological assessment — at multiple timepoints across childhood. Altogether about 4,000 pieces of information were collected on each pregnancy and its outcome.
For the 30,000 children, researchers noted when children were meeting the criteria at the time for various developmental, behavioral and neurological conditions, and also less severe or suspected cases of these conditions. The CPP was particularly thorough in finding even subtle cases that the educational and medical systems would not have captured.
The following criteria were used for assigning a child with the label of infantile autism. Though many say the criteria for autism were restrictive in the 1960s, I find them remarkably similar to the criteria used when my own two children were diagnosed with DSM-IV Autistic Disorder many decades later. They included the presence of the following characteristics by age three:
Abnormal responses to external stimuli: a pattern of marked under- or over-responsiveness noted by outside observers;
Stereotyped or automatic behaviors: hand-flapping, rocking, head-banging, masturbation, twirling, spinning of objects, nose-picking/lip-chewing;
Abnormal affective human contact: marked bizarreness in relating, including poor eye contact, preference for objects over people, extreme withdrawal from people; and
Abnormal language development: echolalia, use of unconnected words and phrases, irrelevant speech, perseveration, adoption of jargon, making bizarre sounds, clang associations.* (*Editor’s note: clang associations = groups of words chosen because of the catchy way they sound, not because of what they mean.)
From Torrey et al. Journal of Autism and Childhood Schizophrenia, 5(4):288-297 (1975).
Based on the CPP’s thorough developmental assessments, what was the rate of identified autism cases? According to the paper by Torrey and colleagues, at age 7, the rate for infantile autism was .0466%, reflecting 14 of 30,000 children who were followed up, or 1 out of 2,143 children, which was consistent with numbers from UK studies at that time. The sex ratio was 4 to 1 males to females, consistent with ratios seen then, and today. Half the children were black, five were white, and one from Puerto Rico and one from India, a rate comparable to the overall study population, which was more heavily black and less white than the U.S. population as a whole.
Of the 14 autistic children, at age 7, three had IQ scores above 70 (71, 72, 73), four had scores below 70 (37, 45, 50 and 50), and seven were considered untestable. Therefore, by today’s standards for intellectual disability (IQ of 70 or less), only 11 children in the CPP cohort had autism with ID, or .0366% of the population. But let’s stick with the full 14 for the sake of being conservative when comparing to today’s rates of autism with ID.
Now, the Torrey paper also identified six additional CPP children who were labeled as severely disturbed, apparently psychotic, childhood schizophrenic or possibly autistic. Four had abnormal language development and abnormal affective human contact when younger, but at age 7 had normal neurological development. The other two children were said to be obviously abnormal. The IQs in this group were 54, 67, 78, 82, and two were not testable. So, for the sake of constructing an even more conservative comparison to autism today, let’s add all those into the CPP autism pile, for a total of 20 children out of 30,000, or a rate of .066% cases of classic autism.
Torrey et al. admitted that they may not have captured every case of what we today would call classic autism, but they stated they believed most of the autistic children were identified.
I hope it is plain to all readers that the rate of classic or severe autism is much, much higher than .066% today.
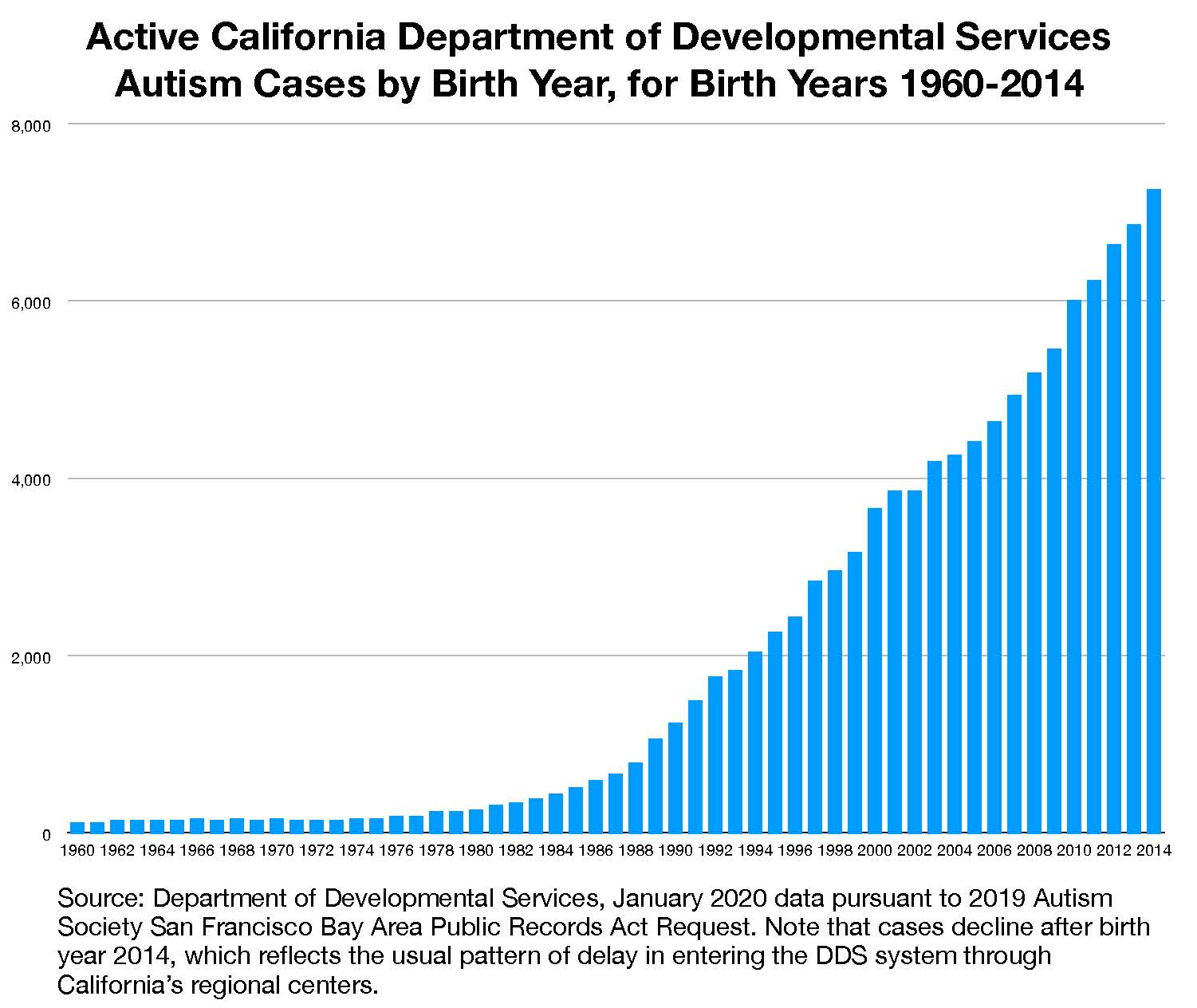
As one point of comparison, let’s look at California Department of Developmental Services (DDS) autism cases, which is limited to more severe forms of autism, involving intellectual disability and functional impairments. Most of these cases would meet the Torrey criteria. The prevalence of DDS-eligible autism has recently surged past a shocking 1% of all children born in the state, which is 15-fold higher than the CPP’s .066%.
Did the researchers who so thoroughly evaluated the CPP children miss about 300 cases of classic autism (that is, 20 identified cases x 15)? I find that difficult to believe — how did the CPP classify the missing 300 cases? Simply as intellectual disability? There is no indication of this. In fact, at age 7, the CPP rate of severe intellectual disability (then called mental retardation) was 0.6%, which as I understand it, meant approximately IQ 70 and under (in the CPP, the values differed depending on sex and race). This is about the same rate seen in CDC autism cases today — but the CPP’s .6% encompassed ALL cases of low IQ —not just autism, but also chromosomal and genetic disorders such as Down Syndrome, all hypoxia at birth, all encephalitis, all brain injuries, etc. Therefore, it seems impossible that the rate of autism with ID was the same as today.
A comparison to U.S. Centers for Disease Control autism data is also in order. According to the CDC’s ADDM network, of the approximately 1 in 54 U.S. children with ASD today, 33% have intellectual disability, with low IQ ≤ 70. (In addition, 24% have borderline intellectual disability, with IQs of 71-85, and 42% have IQs above 85.) (Maenner et al. 2020).

A review of data from the CPP archives would enable us to fill in the knowledge gaps about the magnitude of the autism increase over the past five decades, even if limited to an apples-to-apples review of obvious cases of classic autism.
That means about .61% of U.S. children today have autism with significant ID. Even limiting autism to a narrow low-IQ definition, the rate today is still 9.2-fold higher than in the .066% autism rate of CPP era (which included IQs higher than 70). Using the full 1 in 54 rate, the U.S. autism rate is 28-fold higher than the CPP autism.
Now referencing only the rate in the CDC’s autism with low-IQ subset, did the researchers who so thoroughly evaluated the CPP children miss about 180 cases of autism (that is, 20 identified cases x 9.2)? Again, per the discussion above I find that difficult to believe.
Furthermore, of the 40,000 CPP children for whom there is this data, only about 125 children were institutionalized, for total of .31% of children. This would have included many with Down Syndrome, CP, epilepsy, brain injury, and rare genetic disorders, in addition to autism. While many argue that autism was “hidden” in previous generations due to mass institutionalization, the CPP data does not bear this out.
A moral imperative: Ascertaining autism cases in the CPP
Now, I am not an epidemiologist, and I admit that my analysis here is a back-of-the-envelope approximation attempting to compare apples to apples between children of the 1960s and today. But combing through the detailed CPP data any reasonably skilled epidemiologist or clinician could determine past autism rates by today’s standards. And if that might be difficult for high-functioning autism, it’s at least possible with regard to the more clearly impaired subset. This objective comparison would require knowing intellectual, social, behavioral and adaptive functioning of the children — and that data exists, in spades.
An analysis should eschew any fixation about labels and instead focus on objective, qualitative measures, such as that for adaptive functioning. Measurement of skills needed in normal daily living is, after all, the essential nub of the autism crisis today — our concern is for the growing ranks of mentally disabled children who will never be able to care for themselves (no matter what the diagnostic label). There are also ways to objectively measure intellectual skills, communication and language skills, capacity for abstract thought, and social skills, among others.
“We have the moral duty to discover the truth about the decline in mental functioning among U.S. children.”
Have we in fact been experiencing a significant decline in mental functioning among our children? If so, this implies dramatic shifts in research priorities and long-term care policy and funding. America, we have the ability, and the moral duty, to discover the truth once and for all. Let’s do this.
[I must add my constant refrain when discussing these rising rates — vaccines do not cause autism. Please vaccinate your children.]
Jill Escher is an autism research philanthropist and president of the National Council on Severe Autism. She is also the parent of two children with nonverbal forms of autism.
Disclaimer: Blogposts on the NCSA blog represent the opinions of the individual authors and not necessarily the views or positions of the NCSA or its board of directors.